Understanding information needs during the patient journey: ovarian cancer

While patients see physicians as the primary and most trusted information resource, research indicates that patients with cancer also seek information elsewhere. Reasons for investigating further include 1) verification or double checking, 2) clarifying what they have learned and even obtaining translations of what they have heard from other patients who have “been there,” 3) being directed by one source to query another source1 and for those who reach out to other patients 4) trust and desire for real world experience in managing expectations.
Recent studies on cancer information-seeking focus on the content sought, the level of involvement and the timing of information seeking as it relates to the patient journey.
In one study, researchers scraped Reddit for cancer content in one of its discussion communities. A content analysis provided some suggestions of the informational and emotional needs of cancer patients.2
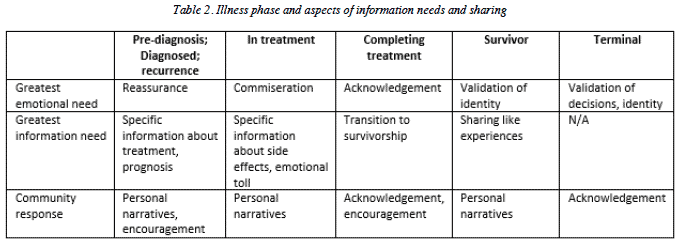
2 Jordan, E., Zakariya, D. & Pratt, W. (2015). Self-Characterized Illness Phase and Information Needs of Participants in an Online Cancer Forum. Proceedings of the Ninth International AAAI Conference on Web and Social Media http://www.aaai.org/ocs/index.php/ICWSM/ICWSM15/paper/download/10546/10493
Taking this framework and using Insight Discover strategies, we focused on the ovarian cancer journey to provide more details about the information needs of patients as they proceed through their journey. This pilot study involved a review of over two hundred publicly available posts and comments from the Ovarian Cancer Support Community on Inspire. The community, with over 46,000 members, was created in partnership with the Ovarian Cancer Research Alliance.
We used keywords and questions to search for patient content along general stages of a cancer journey, de-identified and analyzed postings to obtain insights into the information seeking behavior within each stage.
Pre-diagnosis: Experiencing symptoms
Because the symptoms of ovarian cancer are often described as vague, less than 20% of ovarian cancers are caught in early stages.3 Experiencing symptoms but not being believed or being misdiagnosed commonly occurs for women who ultimately receive an ovarian cancer diagnosis. In this post, an Inspire community member describes her search for a diagnosis.
“Is it possible that ovc can be missed on CT scan & abdominal ultrasound? I’m having just about all the early symptoms -bloated, get full fast, nauseous everyday, left abdominal & lower back pain, heavy bleeding, frequent urination…change in bowels, and fatigue….All my tests are coming up normal …but I know something is wrong…. They’re making me feel crazy (like I’m a hypochondriac) maybe I am”
Responses included finding another physician, doing the lab test yourself and remembering to believe in yourself.
“You know your body and know that something is not right. Just because they can’t find it, does not mean nothing is wrong. Hang in there and advocate for yourself.”
Information Needs and Recommendations: Women need a list of the symptoms of ovarian cancer and they also need a list of the tests used to confirm a diagnosis of ovarian cancer. Information that women need when experiencing symptoms include the names of the types of specialists to go to for testing. Likewise, women require content which supports personal advocacy including self-talk that bolsters this advocacy. They also have need of a list of questions to ask a specialist.
Diagnosis and Pre-Treatment
“Hi everyone ….I was just diagnosed…with ovarian cancer. I don’t know what stage yet but have the ball rolling with appointments next week on the plan and surgery in [number of] weeks. I am [age] and scared to death! I…am desperately looking for positive vibes from anyone!”
Responses included reassurance that being afraid is a normal response.
“I have been diagnosed with an aggressive ovarian cancer that so far has spread only to the [part of the body]. I will meet with an oncologist this [day]. Has anyone out there had a similar situation? If so, what did you do for it? …anyone have any idea how long I can hope to live with surgery and chemo? No one seems to want to tell me…”
Another member wondered about genetic testing after receiving her diagnosis.
“I have never had any genetic testing done so I have a couple of questions. Where do you go to have it done from your pcp or your oncologist and how do you know which one? Do most insurances pay for these tests? I really want to have this done I have a …daughter who I am very concerned about.”
Information Needs and Recommendations: As other research has shown, at both diagnosis and recurrence, patients need a significant amount of information that is organized and not overwhelming.
The comments of women in this stage reflect the uncertainty and lack of understanding of the process after receiving a diagnosis. Their needs include a basic explanation of the standard of care at this time. In this case, standard of care includes, pre-surgery chemotherapy, debulking surgery and post-surgery chemotherapy. Each of these three segments of initial treatment requires a clear explanation of the types of chemotherapy that are used along with the side effects and what is removed during a debulking surgery.
Neoadjuvant chemotherapy
Specifically, neoadjuvant chemotherapy is not recommended for all cancers but research indicates that ovarian cancer outcomes improve with this treatment prior to debulking surgery. There is need for this information to be explained to both patients and caregivers.
Surgery
Several posts requested information on what is removed during debulking surgery. These posts indicate some confusion as to the purpose of this amount of surgery and why exploratory surgery might be necessary.
Chemotherapy after surgery
Information that can set expectations for the first line chemotherapy treatment and the timeline can ease some of the uncertainty that patients feel at this time.
Genetic testing
Around 10 to 15 percent of women who develop ovarian cancer have a mutation in either
their BRCA1 or BRCA2 genes. These and other genetic mutations can impact patient treatment and susceptibility to other cancers. It can also impact family members who may have inherited the mutation, increasing their risk of breast and ovarian cancer.It is apparent from this posting that basic information is needed around where to get genetic testing, who does genetic testing and the reasons for genetic testing.
At this stage, patients need to have an understanding that their best care would be with a specialist called a gynecological oncologist and that there are centers of excellence in the treatment of ovarian cancer around the country. A list of centers should be provided.
Additionally, definitions of terminology that are unfamiliar to patients would be helpful: like ascites, serous, undifferentiated cells, differentiated cells, metastases as well as other “medicalese” found in pathology reports. A full description of what ovarian cancer staging means to treatment but not a discussion of prognosis would be useful.
Among the reviewed postings were questions from younger women. For younger patients, information should include a discussion of fertility preservation and the importance of making sure that their physician has fertility preservation in mind. Women of childbearing age may also require information on breast feeding and options if they receive their diagnosis during or immediately after childbirth.
Patients also need supportive communications that fear is expected and normal. Further, they may need a “how-to” on explaining the diagnosis to family. Because there is a hereditary element to ovarian cancer, the importance of discussing the diagnosis with other women in the family may also be in order.
Information about maintaining a healthy lifestyle, including nutrition, exercise, meditation and counseling would be useful at this time and throughout the patient journey.
Although the time-frame may be short, activating a support system or researching resources will be helpful. Facilitate this effort with a “how to” ask for support and a list of support services that are available for people with cancer.
Finally, as one commenter posted:
“Steer clear of googling too much as some statistics are outdated and will scare you. This board is great for …debunking the myths.”
This is an important statement and is related to comments of patients about “anticipatory grief.” Prognostic data on ovarian cancer may be outdated and does not reflect the individuality of responses to treatment. Unfortunately, because of the poor prognosis numbers “out there,” women receiving this diagnosis may believe they are about to die and may be surrounded by family and close friends with this same misconception. Information should focus on the individuality of responses and provide stories of long-term survival to counterbalance this negative framing of an ovarian cancer diagnosis.
In Treatment
When a caregiver asked about the pain experienced by his loved one during her third dose of neoadjuvant chemotherapy, members responded,
“it’s very likely the [type of chemotherapy medication] causing the numbers and pain. Not much helps except pain meds. The more doses of [type of chemotherapy medication], the greater the odds she will get neuropathy and bone pain.”
Another caregiver responded,
“Joint pain after chemo seems to last 4-5 days before letting up for my [loved one]. The numbness (neuropathy) is worst the first week and then fades between treatments. …Make sure [your loved one] is communicating her numbness each week. On a scale of 1-10. Is it getting better, worse, etc. Your doctor will want to know …As you will read on this board from many others, the chemo has a cumulative effect. It’s a tougher hill each time through the cycle but it also means the drugs are doing their job.”
Information Needs and Recommendations: Patients and caregivers need information on side effects of neoadjuvant chemotherapy, what to expect, treatments for side effects and the importance of reporting those side effects. There are moisturizers for skin, treatments for mouth sores and recipes for stomach symptoms that would be useful at this stage. Patients and caregivers also need information for treating pain, especially about treating pain immediately at onset to stop the cycle of pain.
“I am [age] and I just had my second ovary removed due to …recurrence. That of course put me into early menopause. So far I have been getting hot flashes and they are pretty consistent. My doctor doesn’t want me on any hormone treatment and I don’t want it either. I am looking for some natural methods of managing those hot flashes.”
Information Needs and Recommendations: Debulking surgery puts women into menopause. Posts requested information on treating menopausal symptoms like hot flashes, dryness and reduced libido.
“I know about worrying about not being able to afford the side costs of medical care. You need to ask your Dr and or your local Cancer resource center about talking with a nurse navigator. Mine was amazing. She not only set me up with free transportation, but she got me reimbursed for $500 I had already spent on driving….She set me up with free meals from a local organization during treatment…I found a program near my out of town hospital…that provides need based “scholarships” for patients and families hotel rooms. …there is a lot of help available for cancer patients. Don’t let $$ determine your care.”
Information Needs and Recommendations: Postings included concerns about how to finance treatment, travel and loss of income. Information about financial resources, cancer navigators and signing up for SSDI would be useful to patients dealing with ovarian cancer and their caregivers.
Completing treatment:
“I finally got my first CT since finishing 18 weeks of chemo [date]. A month seemed so long to wait. Well, the scan showed no visible evidence of disease. My blood test for CA-125 was [number]…. My oncologist does not have me scheduled for regular CT scans. She will have me do bloodwork every 3 months. She said research does not support continued scans and that she will do one if I am experiencing symptoms. Otherwise, she said why subject me to more radiation, and why do it if the research shows that it doesn’t increase survival. What do you all think? Is this how most oncologists follow up? …Please tell me what your follow-ups have been? How frequently? CT, Pet or other scan? CA blood test? I want to feel trusting of my doctor.”
Information Needs and Recommendations: Along with the congratulatory communication that patients desire and deserve in completing initial treatment and hopefully attaining no evidence of disease
(NED), patients need information on next steps or standards of care around surveillance.
In addition, patients need guidance on dealing with scan anxiety also called scanxiety. Information can include explanations of PTSD and dealing with the emotions around their experience through mental health counseling.
Finally, sharing healthy living tips, nutrition and physical activity can complement provided material.
Recurrence:
“my situation didn’t look too good going in…. that was two years ago and, although I have had one recurrence and have been in constant treatment of one sort or another….I’m telling you all of this because I want you to see that there is life after ovarian cancer. Never lose sight of that. Pick a prize and keep your eye on it! Surround yourself with good people, and be kind to yourself. This is the time for YOU! Respect your feelings, cry if you need to, scream if you need to, because it will all help you come to an understanding and acceptance of your ‘new normal.'”
Information Needs and Recommendations: As with the diagnosis stage, there is significant demand for information. Patients and caregivers need a clear description of the language of recurrence. For example, they may hear that their cancer is [chemotherapy name]-resistant but they do not know what that means. Offering stories of other patients who have achieved lasting remissions after recurrence can be part of the explanation of when cancers become resistant to one form of chemotherapy. Copy can introduce the concept of cancer as a chronic condition being treated as heart disease is treated: instead of dying of cancer, living with cancer. Incorporate resilience training as well as articles on nutrition, physical activity and healthy living in communication.
The message for patients at this juncture is that there are other treatments available. Providing information to patients on what a clinical trial is, why it is not a last resort, where they are located and how to find and apply for one is useful at this time.
As during initial diagnosis, encourage tissue preservation for testing.
Another asset for patients would be plain language medical journal article summaries on recent research on ovarian cancer treatments.
Conclusions
In this review of patient postings, we identified many questions that plain language articles can answer. At diagnosis and throughout their journey, cancer patients experience a flood of emotions and influx of information that can overwhelm. Managing treatment, while attempting to organize and obtain research has been likened to having at least another part-time job. Retreat is an understandable reaction when overwhelmed by fear, anxiety and the physical impact of the disease process and treatment. Health literacy and self-advocacy can be compromised.
Providing support and plain language information in a timely manner for patients and caregivers may lessen the burden of this complicated disease experience. We hope to utilize these preliminary findings to create content that is easy to find, easy to understand and which supports women from pre-diagnosis through all stages of the ovarian cancer patient journey.

Inspire offers a trusted community to patients and caregivers. Our goal with this blog, this website and our content is to provide the life science industry access to the true, authentic patient voice. In so doing, we support faithful operationalization of patient-centricity. Take a look at our case studies, eBooks and news outlet coverage.
References:
1 Nagler, R. H., Romantan, A., Kelly, B. J., Stevens, R. S., Gray, S. W., Hull, S. J., … Hornik, R. C. (2010). How Do Cancer Patients Navigate the Public Information Environment? Understanding Patterns and Motivations for Movement Among Information Sources. Journal of Cancer Education : The Official Journal of the American Association for Cancer Education, 25(3), 360–370. http://doi.org/10.1007/s13187-010-0054-5
2 Jordan, E., Zakariya, D. & Pratt, W. (2015). Self-Characterized Illness Phase and Information Needs of Participants in an Online Cancer Forum. Proceedings of the Ninth International AAAI Conference on Web and Social Media http://www.aaai.org/ocs/index.php/ICWSM/ICWSM15/paper/download/10546/10493
3 http://ovarian.org/about-ovarian-cancer/what-are-the-signs-a-symptoms